

1 Like
Jepp, lower risk movet er å vente på at man får et definitivt brudd oppover, og helst litt momentum på bevegelsen, alt før det er og blir knivfanging i det lange bildet 
4 Likes
Novo Nordisk’s investigational zenagamtide shows significant A1C reductions with up to 14.6% weight loss in adults with type 2 diabetes–presented at ADA 2026
A phase 2 study of investigational once-weekly subcutaneous zenagamtide showed statistically significant reductions in blood sugar in adults with type 2 diabetes compared to placebo, with up to 89.1% achieving A1C below 7%1 Additionally, participants treated with zenagamtide showed body weight loss up to 14.6% at week 36 with the highest dose investigated, 40 mg1 Zenagamtide will advance into phase 3 clinical trials in adults with type 2 diabetes based on these resultsPLAINSBORO, N.J. and BAGSVÆRD, Denmark, June 5, 2026 /PRNewswire/ – Novo Nordisk today announced new clinical data from the positive phase 2 trial of investigational zenagamtide, also known as amycretin. Zenagamtide is the first of its class, being a unimolecular peptide agonist of GLP-1 and amylin receptors.1 Presented at the 2026 Scientific Sessions of the American Diabetes Association® (ADA) in New Orleans, LA, results from the phase 2 dose finding study included the evaluation of six subcutaneous doses of zenagamtide (ranging from 0.4 mg to 40 mg) versus matched placebo in 262 adults with type 2 diabetes inadequately controlled (A1C 7.0–10.0%) on metformin, with or without an SGLT2 inhibitor. The study met its primary endpoint of change in A1C across all doses and also key supportive secondary endpoint of change in body weight (with doses 1.5 mg and greater) with zenagamtide versus placebo after 36 weeks.1
“Zenagamtide is the first investigational treatment for type 2 diabetes to combine GLP-1 and amylin receptor agonist mechanisms of action in a single molecule. These phase 2 results build on the growing body of evidence which demonstrates the potential of zenagamtide to meaningfully impact blood glucose control in patients with type 2 diabetes and also body weight,” said Martin Holst Lange, chief scientific officer and executive vice president, Research & Development at Novo Nordisk. “These results underscore our scientific leadership and position us to continue advancing innovative treatment options that could expand the therapeutic landscape and provide patients and healthcare professionals with greater choice in managing type 2 diabetes.”
The phase 2 study showed a dose-dependent and statistically significant change in A1C from baseline to week 36 with all doses vs placebo. From a baseline of 7.8%, the estimated mean change in A1C at week 36 was up to ‒1.71% with zenagamtide 40 mg (estimated treatment difference [ETD] vs placebo: ‒1.56% [95% confidence interval (CI): ‒2.05, ‒1.07]; p<0.0001).1 Up to 89.1% of participants on zenagamtide achieved A1C levels below 7%, and up to 76.2% achieved levels at or below 6.5%.1 Notably, the proportion of time spent within target range of 70–180 mg/dL (3.9–10.0 mmol/L) was above the internationally recommended target of >70% across all zenagamtide doses investigated (up to 91.5% with zenagamtide 40 mg).1 These results suggest strong glycemic efficacy, considering that the higher zenagamtide dose treatment groups were only exposed to the maintenance dose for a short period of time (ie 20 mg for 8 weeks and 40 mg for 4 weeks).1
As a key supportive secondary endpoint, trial participants taking zenagamtide also saw a mean body weight reduction of up to 14.6% (baseline body weight ~219 lbs) with the 40 mg dose compared with 2.1% with placebo.1 No apparent weight loss plateau was seen at week 36 with the higher doses of zenagamtide.1
Table. Endpoints: once-weekly subcutaneous zenagamtide vs placebo
Once-weekly subcutaneous zenagamtide
Participant (N=262) baseline characteristics: Male 66%; mean age 57.1 yrs; A1C 7.8%; body weight 99.2 kg (218.7 lbs); 40% on SGLT2i.
All patients on a stable dose of metformin with or without SGLT2 inhibitor.
Each endpoint was analyzed using an ANCOVA model. The analyses were based on data from the on-treatment without rescue medication observation period.
Using the dose–response model for analysis, the estimated mean change in A1C from baseline to week 36 was up to –1.8% (ETD vs placebo [95% CI]: –1.58 [–2.08, –1.08]; p<0·0001); the estimated mean change in body weight was up to –14.5% (ETD vs placebo [95% CI]: –11.81 [–15.37, –8.25]; p<0.0001), with zenagamtide 40 mg.
This trial used a fixed-dose-escalation trial design; if the planned treatment dose was not tolerated, treatment was permanently discontinued.
In the trial, the most common adverse events were gastrointestinal, and the majority were mild to moderate in severity. The safety and tolerability profile in this phase 2b trial was consistent with other incretin and amylin-based therapies. These results support further investigation of zenagamtide in phase 3 trials.1
Based on the results, Novo Nordisk is planning to initiate a phase 3 development program with zenagamtide for adults with type 2 diabetes in H2 2026.

Er vel denne som ikke ser helt bra ut:

Flere postere vil dukke opp her:
https://sciencehub.novonordisk.com/congresses/ada2026.html
UBT251:

Og bilder av noen slides fra x:

.

3 Likes
Voldsomt med bivirkninger på zenagamtide. 20 og 40 mg blir nok for heftig, diabetes er en folkesykdom, kan ikke ha så mye bivirkninger som det der.
UBT251 ser dog mye mer lovende ut! Den kan absolutt konkurrere med Retatrutide for fedme👍
Spørsmålet her er vel om de har økt for fort. Og om mange flere kunne blitt holdt i trial om man hadde vært mer fleks. Men Novo gjorde jo det med CagriSema, og resultatet ble jo at selskapet selv + investorene egentlig ikke helt vet hvor bra / dårlig produktet egentlig er. Når det er sagt så begynner vi å se at GLP-1 + amylinagonist som targeter calcitoninreseptor ikke akkurat gir utmerket toleranse. Kan se ut som LLY traff veldig bra med 1:1 GLP-1 og GIP i tirzepatide. GIP-agonisten ser rett og slett ut til å motvirke en del AE’s.
Vi får se om Novo finner ut at de vil lage seg en “basisdrug” med ca. samme egenskaper. Kan være de henter sin egen double agonist ned fra hylla. Eller kanskje kjøper en. Har tidligere skrevet at Novo neppe ville være interessert i VKTX pga egen pipe. Men slik pipen til Novo utvikler seg nå, så kan en godt balansert GLP1/GIP-agonist i bakhånd være en smart move.
2 Likes
Flere press releases fra ADA
People with type 2 diabetes who were increased to semaglutide 2 mg were as likely to achieve an HbA1c less than 7% and more likely to achieve greater than 5% weight loss than those who were switched to tirzepatide, in real-world data
Adults with type 2 diabetes on semaglutide 1 mg whose dose was increased to 2 mg were as likely to reach an HbA1c level <7% and were more likely to see weight loss of ≥5% vs those who were switched to tirzepatide 2.5 mg or 5 mg with allowed titration up to 15 mg1
This retrospective claims analysis, across >64,000 US adults, offered exploratory insights of patients with type 2 diabetes who were escalated from 1 mg to 2 mg semaglutide vs switching to tirzepatide, in a real-world dose titration1
PLAINSBORO, N.J. and BAGSVÆRD, Denmark, June 6, 2026 /PRNewswire/ – Novo Nordisk today announced new real‑world evidence in adults with type 2 diabetes (T2D) treated with once‑weekly semaglutide 1 mg that examines how escalating to semaglutide 2 mg compares with switching to tirzepatide and supports patient goals for HbA1c and weight loss. By one year, both groups were associated with similar proportions of patients achieving an HbA1c of <7%, and people on semaglutide 2 mg had a statistically significant higher event rate for achieving weight loss ≥5% when compared to people switching to tirzepatide (starting on 2.5 mg or 5 mg with the ability to titrate).1 This retrospective cohort analysis, drawn from a large US claims database (January 2018-September 2025), supports escalating to semaglutide 2 mg as a clinically appropriate and effective treatment strategy.1 These findings will be presented at the 2026 Scientific Sessions of the American Diabetes Association ® (ADA) on Sunday, June 7.
“These data analyzed an important clinical consideration: for patients already on semaglutide therapy, dose escalation of current therapy may get patients to their treatment goals compared to transitioning to a different therapy,” said Michael Radin, MD, Executive Medical Director at Novo Nordisk Inc. “These real-world findings directly support the established ADA guidelines, which recommend that many adults with type 2 diabetes strive for an HbA1c under 7% alongside at least a 5% to 7% reduction in body weight.”
For blood glucose outcomes, results from the cohort of >64,000 adults living with T2D (escalated to semaglutide 2 mg, n=55,550; switched to tirzepatide, n=9,338; baseline HbA1c: 7.2%) showed comparable rates of patients reaching an HbA1c <7% by one year were observed with both semaglutide 2 mg and tirzepatide. By one year, 74.7% (95% CI: 73.3%–76.2%) of adults who were escalated to semaglutide 2 mg achieved HbA1c <7% compared with 75.1% (95% CI: 74.0%–76.2%) who switched to tirzepatide (P<0.001). Adults in both groups were similarly likely to achieve an HbA1C <7% over the time variable follow‑up period (estimate: 0.98; 95% CI: 0.94–1.02; P=0.343).1
In terms of weight loss, in a cohort of >56,000 adults living with T2D (escalated to semaglutide 2 mg, n=48,596; switched to tirzepatide, n=8,256), the analysis found that people on semaglutide 2 mg had a higher event rate for achieving weight loss ≥5% compared to people switching to tirzepatide (starting at 2.5 mg or 5 mg with ability to titrate), from a baseline of 105 kg and 106.2 kg, respectively.1 By one year, 60.5% (95% CI: 58.7%–62.3%) of adults who escalated to semaglutide 2 mg achieved ≥5% weight loss compared with 55.3% (53.9%–56.7%) who switched to tirzepatide (P<0.001). Adults who escalated their dose also had a higher likelihood of achieving ≥5% weight loss over time (HR 1.19; 95% CI 1.15–1.24; P<0.001), underscoring a statistically significant difference for dose escalation in this real‑world analysis.1
Across both HbA1c and weight loss cohorts, after switching to an initial tirzepatide dose of either 2.5 mg or 5 mg, clinicians had the flexibility to titrate across the tirzepatide dosing regimen, where approximately 24% of the HbA1c cohort and approximately 40% of the weight loss cohort reached doses of tirzepatide that were >5 mg and approximately 3%-5% reached tirzepatide 15 mg.1
“These real‑world findings offer useful perspective on how we think about intensifying therapy for adults with type 2 diabetes who may need additional glycemic control,” said Kathryn S. Tierney, MSN, APRN, FNP-BC, FAANP, Middlesex Health MultiSpecialty Group in Middletown, CT. “In practice, many patients already on semaglutide may prefer to build on that foundation rather than start over with a new medication. The potential to reach blood glucose goals with meaningful weight loss makes maximizing semaglutide escalation a sensible, patient-focused approach for healthcare professionals and patients to discuss.”
Real-world study data can provide valuable insights into how treatments work outside of controlled clinical trial settings. Real-world data analyses also have several limitations; results may reflect residual unmeasured confounding, while associations can be demonstrated, causal relationships cannot be definitively established. Additionally, use of retrospective claims data may exclude patients with intermittent coverage or underserved populations, potentially limiting generalizability.
About COMPETE SWITCH
COMPETE SWITCH is a retrospective cohort study using Komodo Health’s Healthcare Map with linked laboratory results, a large US healthcare claims database (January 2018– September 2025), which evaluated the dosing and titration of semaglutide and tirzepatide in a real-world setting. Patients included were adults with type 2 diabetes with a prescription claim for semaglutide 1 mg with subsequent claims for either semaglutide 2 mg or tirzepatide 2.5 mg or 5 mg. The study included 64,888 adults in an HbA1c cohort and 56,852 in a weight‑loss cohort. As with all observational analyses, the findings have inherent limitations and may not fully translate to all clinical settings. While many patients have HbA1c and weight information, not all do, limiting the ability to characterize those patients who do not. Additional limitations exist in the ability to characterize or describe social determinants that may impact medication adherence or influence switching. There is no reason to suspect these differences will differentially bias the results.1
Novo Nordisk to present new data on Wegovy® across a wide range of cardiometabolic conditions at the American Diabetes Association’s 2026 Scientific Sessions
Post hoc analyses explored the impact of semaglutide across an array of conditions including obstructive sleep apnea (OSA), asthma-related adverse outcomes, liver health, cardiometabolic risk factors, and other obesity-related comorbidities1-6
Two of the post hoc analyses demonstrated semaglutide use was associated with a reduction of asthma-related adverse outcomes and improvements in systolic blood pressure for those with uncontrolled hypertension and overweight or obesity, respectively2-3
Multiple post hoc analyses were of the SELECT study, the pivotal study which led to an indication to reduce the risk of MACE in adults with obesity or overweight and established cardiovascular disease, along with diet and exercise1-2,7
PLAINSBORO, NJ and BAGSVÆRD, Denmark, June 6, 2026 /PRNewswire/ – Novo Nordisk is presenting post hoc analyses from the SELECT, STEP, ESSENCE, and OASIS clinical trials at the 2026 Scientific Sessions of the American Diabetes Association® (ADA), highlighting data regarding the impact of semaglutide across weight-related conditions.1-6 Across these analyses, findings explore the impact of treatment with semaglutide on obstructive sleep apnea (OSA), asthma-related adverse outcomes, cardiometabolic risk factors, and other obesity-related complications.1-6
“These new analyses build on the growing body of clinical evidence for semaglutide, an important medicine that has already been extensively studied not only in obesity but also in cardiovascular disease and metabolic dysfunction-associated steatohepatitis (MASH),” said Andrea Traina, Pharm.D., senior medical director, Obesity and Liver Health, Novo Nordisk. “We’re continuing to invest in deepening our understanding of the potential for semaglutide to better serve appropriate patients across a diverse set of obesity-related complications.”
These exploratory data add to the growing body of evidence showing obesity is linked to a wide range of interconnected health risks and that treatment with semaglutide in these settings was associated with improved health measurements beyond weight loss alone.
“Obesity is a chronic disease that can cause many complications in the body, contributing to serious comorbidities and broader health issues,” said Domenica Rubino, MD, founder and director, Washington Center for Weight Management & Research. “These analyses, across the spectrum of clinical trial programs conducted to evaluate semaglutide, add to our understanding of the critical ways semaglutide may impact those complications, with the goal of going beyond weight loss to improvements in overall health.”
It is important to note that semaglutide injection 2.4 mg and semaglutide tablets 25 mg contain a Boxed Warning for possible thyroid tumors, including cancer, and should not be used in those with a personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). The most common side effects include nausea, diarrhea, vomiting, constipation, stomach (abdomen) pain, changes in skin sensations, headache, tiredness (fatigue), upset stomach, dizziness, feeling bloated, belching, low blood sugar in people with type 2 diabetes, gas, stomach flu, heartburn, and hair loss.7
Incidence of obstructive sleep apnea
A post hoc analysis of the SELECT trial assessed the impact of semaglutide injection 2.4 mg on risk of MACE in participants with reported OSA as well as incidence of OSA. A questionnaire identified OSA at baseline and incident OSA was captured via adverse event reporting in those without OSA at baseline. At baseline, 2,550 participants (14.5%) reported having OSA.1Semaglutide injection 2.4 mg was associated with a significantly lower incidence of obstructive sleep apnea (HR [95% CI]=0.48 [0.31-0.74]) in adults with overweight or obesity and established cardiovascular disease, compared with placebo.1 Among those without OSA at baseline, there were a total of 95 incident cases of OSA (semaglutide 2.4 mg: 30; placebo: 65). Semaglutide injection 2.4 mg was also associated with a reduced risk of major adverse cardiovascular events (MACE) regardless of OSA status (Interaction p = 0.203.).1
Asthma-related adverse outcomes
In a separate post hoc analysis of the SELECT trial, patients with self-reported asthma were followed for asthma-related AEs/SAEs. A total of 1190 patients had asthma. Overall, patients with established cardiovascular disease, asthma and obesity or overweight treated with semaglutide injection 2.4 mg had a lower incidence of asthma-related AEs/SAEs (n=27) versus placebo (n= 46) [HR 0.58 (95% CI 0.36, 0.93)].2 Changes in biomarkers that reflect inflammation were also evaluated from baseline to week 104; there was a reduction in high sensitivity C-reactive protein (hsCRP) of 38.9% from baseline observed in patients taking semaglutide injection 2.4 mg, with no changes in blood eosinophil or neutrophil counts.2Blood pressure outcomes
In a post hoc analysis including 597 adults with overweight or obesity and with uncontrolled hypertension from STEP 1,3, 5-9 and OASIS 4 clinical trials, semaglutide injection 2.4 mg, along with diet and exercise, was associated with meaningful improvements in systolic blood pressure compared to placebo. From baseline to week 68, significant changes in systolic blood pressure (estimated treatment difference [ETD] –5.48 mmHg, 95% CI –7.78, –3.19; p<0.0001) and diastolic blood pressure (ETD –2.73 mmHg, 95% CI –4.19, –1.27; p=0.0003) were seen with semaglutide injection 2.4 mg compared with placebo in the pooled STEP trial data.3Liver health
In a post hoc analysis of part 1 of the ESSENCE trial of the first 800 participants randomized, semaglutide injection 2.4 mg resulted in consistent improvement in cardiometabolic risk factors (HbA1c, body weight [BW], waist-to-height ratio [WtHR], systolic and diastolic blood pressure [BP], triglycerides, non-HDL cholesterol, hsCRP) and liver health parameters including ALT, controlled attenuation parameter, Enhanced Liver Fibrosis, FibroScan-AST, liver stiffness measurement) versus placebo up to week 72, regardless of baseline glycemia level in people with MASH and liver fibrosis.4 In a separate post hoc analysis of the STEP 1 trial, people with overweight or obesity treated with semaglutide injection 2.4 had a reduction in fatty liver index scores from baseline to week 68.5Cardiometabolic effects of semaglutide in OASIS 4 participants by body mass index class
In a post hoc analysis of the OASIS 4 trial assessing the effect of semaglutide tablets 25 mg on cardiometabolic outcomes (eg, body weight, waist circumference HDL, and LDL cholesterol, HbA1c, blood pressure, fasting plasma glucose, and hsCRP) by baseline BMI class, patients with overweight/obesity class I (BMI 27-<35, n=85) treated with semaglutide tablets 25 mg had similar or greater improvements in cardiometabolic outcomes compared with the obesity class II/III cohort (BMI >=35, n=119) at week 64.6 By week 64, 27% of patients in the overweight/obesity class I cohort were in the National Institute for Health and Care Excellence low health risk category (based on waist to height ratio) versus 2% of the obesity class II/III cohort.6Exploratory post hoc analyses are hypothesis generating, and further work investigating the clinical validity of these results would be of value. Semaglutide is not approved to treat obstructive sleep apnea, asthma, hypertension, or MASLD. Safety and efficacy for these conditions have not been established.
About STEP
The STEP program included phase 3 trials evaluating once-weekly injectable semaglutide, along with diet and exercise, for weight management in adults with overweight or obesity.8About OASIS 4
OASIS 4 was a 64-week phase 3 randomized, double-blind, placebo-controlled trial evaluating the efficacy and safety of once-daily oral semaglutide 25 mg versus placebo in 307 adults with obesity (BMI ≥ 30 kg/m2) or overweight (BMI ≥ 27 kg/m2) with one or more weight-related comorbidities. People with diabetes were excluded. OASIS 4 included a 64-week treatment period, including a 12-week dose escalation, and a 7-week off-treatment follow-up period.9In total, 307 participants were randomized in a 2:1 ratio to once-daily oral semaglutide 25 mg or placebo, alongside lifestyle intervention for 64 weeks.9
About SELECT
SELECT was a multicenter, randomized, double-blind, placebo-controlled, event-driven superiority trial designed to evaluate the efficacy of semaglutide 2.4 mg versus placebo as an adjunct to cardiovascular standard of care for reducing the risk of major adverse cardiovascular events (cardiovascular death, non-fatal heart attack, or non-fatal stroke) in adults with established CVD with overweight or obesity with no prior history of diabetes.10 In SELECT, established CVD was defined as a prior heart attack, prior stroke, or symptomatic PAD.10The trial, initiated in 2018, enrolled 17,604 adults and was conducted in 41 countries at more than 800 investigator sites.10
About ESSENCE
ESSENCE is an ongoing phase 3 trial evaluating the effect of once-weekly subcutaneous semaglutide 2.4 mg in adults with MASH with moderate-to-advanced liver fibrosis (stage F2 or F3). It is a two-part trial in which 1,197 planned participants were randomized 2:1 to receive semaglutide 2.4 mg or placebo, on top of standard of care for 240 weeks.11In part 1, the objective was to demonstrate that treatment with semaglutide 2.4 mg improves liver histology at 72 weeks compared with placebo, based on biopsy sampling from the first 800 randomized patients. In part 2, which is ongoing, the primary objective is to demonstrate that treatment with semaglutide 2.4 mg lowers the risk of liver-related clinical events compared to placebo in adults with MASH and moderate-to-advanced liver fibrosis at 240 weeks.11
Wegovy® pill prescriptions surpass 3 million, 1 filled roughly every 5 seconds, bringing GLP-1 therapy to people with obesity previously untreated, while Novo Nordisk unveils new data at ADA 2026
Three million prescriptions for Wegovy® pill since launch on January 5th serves as another milestone in one of the strongest US pharmaceutical launches by volume on record1
The majority of new Wegovy® pill prescriptions are for people new to GLP-1 therapy, bringing obesity medicine to many previously untreated1
This news comes as Novo Nordisk has a large presence at the American Diabetes Association’s 2026 Scientific Sessions, including a variety of Wegovy® analyses in adults with obesity
PLAINSBORO, N.J. and BAGSVÆRD, Denmark, June 7, 2026 /PRNewswire/ – Novo Nordisk today announced Wegovy® (semaglutide) tablets 25 mg has surpassed three million prescriptions in just over five months, establishing Wegovy® pill as one of the strongest US pharmaceutical launches by volume on record.¹ The three million milestone corresponds to one prescription filled roughly every five seconds, reflecting continued uptake since Wegovy® pill became available in January 2026. Further underscoring its rapid adoption, Wegovy® pill reached its initial one million prescription milestone just 12 weeks after reaching US pharmacies and online providers (week of 1/5/26 to week of 3/23/26), with an additional two million prescriptions accumulated in an even shorter span of just 10 weeks (week of 3/23/26 to week of 6/1/26). The majority of new prescriptions filled for Wegovy® pill (more than 80%) are for people new to GLP-1 therapy, indicating the oral formulation is expanding the obesity treatment market, rather than replacing existing therapies.¹
“Wegovy® offers adults with obesity significant weight loss, along with diet and exercise, and is FDA-approved to lower the risk of major cardiovascular events such as death, heart attack, or stroke in adults with obesity with known heart disease – making Wegovy® pill truly distinct. With Wegovy® pill and Wegovy® HD available for weight management, patients and their healthcare providers are making choices that fit their needs, resulting in the clear adoption for both treatments,” said Jamey Millar, executive vice president, US Operations of Novo Nordisk. “Novo Nordisk remains determined to continue playing a major part in addressing the global public health challenge of obesity by deeply understanding the needs of those who live with it. That is why we are at ADA 2026 – to talk to patients, healthcare professionals, and investors to present our data but also listen and learn.”
This year, more patients starting a new weight management therapy have filled prescriptions for Wegovy® than any other available obesity medication. Alongside the three million prescription milestone for Wegovy® pill, the recently launched Wegovy® HD (semaglutide) injection 7.2 mg has demonstrated strong uptake in the early days of availability.1
Expanding affordable access to medicines is a priority for Novo Nordisk including the expansion of coverage for those with insurance in the US. Those with commercial insurance coverage can access Wegovy® for as little as $25 per month through existing savings programs.* The recently announced Medicare GLP-1 Bridge builds on these efforts to expand access and will provide eligible Medicare beneficiaries living with obesity access to Wegovy® (semaglutide) injection and tablets for a $50 monthly copay † , beginning July 1, 2026. In addition, Wegovy® is available through a range of access options, including more than 70,000 US pharmacies, NovoCare® Pharmacy, select telehealth providers, and others.
This announcement coincides with Novo Nordisk presenting an array of clinical data at the American Diabetes Association® 2026 86th Scientific Sessions in New Orleans (June 5-8, 2026), including a variety of Wegovy® analyses in adults with obesity.
Novo Nordisk is preparing for the first launches of the Wegovy® pill outside the United States in the second half of 2026, including the recently announced approval and launch in the United Arab Emirates.
Novo Nordisk’s CagriSema 2.4 mg / 2.4 mg demonstrated significant reduction in HbA1cand weight across multiple studies in the REIMAGINE program presented at ADA 2026
CagriSema, a once-weekly investigational treatment that combines a novel amylin analog with a GLP-1 receptor agonist (RA), achieved significant reductions in HbA1c and bodyweight versus comparators across three phase 3 trials in adults with type 2 diabetes (T2D)1-3
Data from the REIMAGINE clinical development program, a series of phase 3 trials evaluating once-weekly CagriSema in adults with T2D across various stages of their disease, were presented at an ADA symposium1-3
Novo Nordisk continues to demonstrate pioneering leadership and scientific innovation through advancing diabetes research
PLAINSBORO, N.J. and BAGSVÆRD, Denmark, June 7, 2026 /PRNewswire/ – Phase 3 results from Novo Nordisk’s REIMAGINE 1-3 trials were presented today, showing significant reduction in HbA1c and weight in adults with type 2 diabetes (T2D). The REIMAGINE trials each met their primary endpoint, demonstrating significant reductions in HbA1c and met their confirmatory secondary endpoints in reduction of bodyweight. The breadth of data was presented during a late-breaking symposium at the 2026 Scientific Sessions of the American Diabetes Association ® (ADA) in New Orleans, June 5–8, alongside the simultaneous publication of REIMAGINE 1 and 2 trial results in The Lancet Diabetes & Endocrinology and the REIMAGINE 3 trial results in The Lancet .1-3 The REIMAGINE clinical program evaluating CagriSema in adults with T2D follows previously published results from the REDEFINE clinical program, evaluating CagriSema in adults with overweight or obesity with and without T2D.
“The REIMAGINE 1-3 studies showed promising results by combining a novel amylin analog with the proven significant effects of semaglutide for HbA1c reduction and weight loss in adults living with type 2 diabetes,” said Martin Holst Lange, executive vice president, chief scientific officer and head of Research and Development at Novo Nordisk. “It was particularly encouraging to see these results consistently demonstrated across the REIMAGINE trials in adults with type 2 diabetes at various stages of their disease, from first-line therapy to add-on to basal insulin. With these robust findings, CagriSema has the potential to be the first amylin and GLP-1 combination therapy that addresses blood glucose control with reductions in bodyweight for people living with type 2 diabetes.”
Amylin, a pancreatic hormone co-secreted with insulin in response to food intake, plays a distinct yet complementary role to GLP-1, with potential roles in appetite, glycemic control, bone metabolism, and bodyweight.4-6
“The therapeutic potential of amylin in type 2 diabetes has been recognized by the medical community for many years,” said John B. Buse, MD, PhD, Distinguished Professor of Medicine, Director of the UNC Diabetes Care Center. “Now, in the REIMAGINE trials, we’re taking that knowledge forward by exploring the combination of cagrilintide, a novel long-acting amylin receptor agonist, paired with semaglutide. This synergistic approach was designed to address multiple pathways of glucose regulation and may potentially offer meaningful benefits for patients who may need a different approach to managing their type 2 diabetes.”
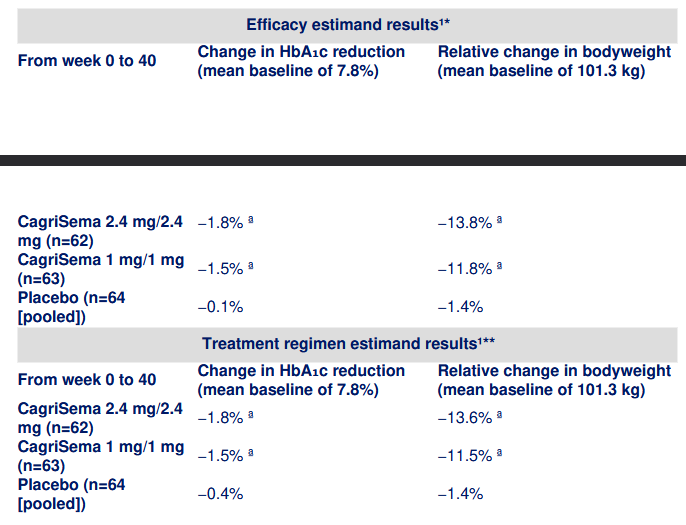
REIMAGINE 1 was a 40-week phase 3 trial evaluating the safety and efficacy of CagriSema in doses 2.4 mg/2.4 mg and 1 mg/1 mg once weekly versus dose-matched placebo in 189 adults with T2D inadequately controlled on diet and exercise. The primary endpoint was change in HbA1c (%-points) from baseline to week 40. Confirmatory secondary endpoints included relative change in bodyweight (%) from baseline to week 40.1
a Statistically significant compared to placebo, estimated mean, p<0.0001
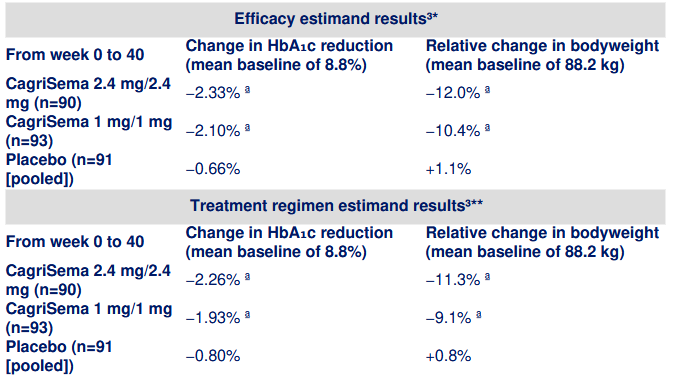
REIMAGINE 2 was a 68-week phase 3 trial evaluating the safety and efficacy of CagriSema in doses 2.4 mg/2.4 mg and 1 mg/1 mg once weekly versus semaglutide 2.4 mg, semaglutide 1 mg, cagrilintide 2.4 mg, and dose-matched placebo in 2,713 adults with T2D inadequately controlled with metformin with or without an SGLT2 inhibitor. The primary endpoint was change in HbA1c (%-points) from baseline to week 68 with CagriSema 2.4 mg/2.4 mg versus semaglutide 2.4 mg. Confirmatory secondary endpoints included additional HbA1c comparisons and relative change in bodyweight (%) from baseline to week 68.2
a Statistically significant compared to semaglutide 2.4 mg (p=0.0035 HbA1c, p<0.0001 bodyweight), cagrilintide 2.4 mg, and semaglutide 1 mg, estimated mean, p<0.0001b Statistically significant compared to placebo, estimated mean, p<0.0001
c Statistically significant compared to semaglutide 1 mg, estimated mean, p<0.0001
d Statistically significant compared to semaglutide 2.4 mg (p=0.028 HbA1c, p<0.0001 bodyweight), cagrilintide 2.4 mg, and semaglutide 1 mg, estimated mean, p<0.0001
e Statistically significant compared to placebo, estimated mean, p=0.0015
REIMAGINE 3 was a 40-week phase 3 trial evaluating the safety and efficacy of CagriSema 2.4 mg/2.4 mg and 1 mg/1 mg once weekly versus dose-matched placebo in 274 adults with T2D as add-on to once-daily basal insulin with or without metformin. The primary endpoint was change in HbA1c (%-points) from baseline to week 40. Confirmatory secondary endpoints included relative change in bodyweight (%) from baseline to week 40.3
a Statistically significant compared to placebo, estimated mean, p<0.0001.In the REIMAGINE 1 trial, the most commonly reported adverse events (AEs) were gastrointestinal (GI)-related, occurring in 33/62 (53%) participants in the CagriSema 2.4 mg/2.4 mg group, 28/63 (44%) participants in the CagriSema 1 mg/1 mg group, and 13/64 (20%) participants in the placebo group. AEs leading to trial product discontinuation occurred in 2/62 (3%) participants in the CagriSema 2.4 mg/2.4 mg group, 2/63 (3%) participants in the CagriSema 1 mg/1 mg group, and 2/64 (3%) participants in the placebo group.1
In the REIMAGINE 2 trial, the most commonly reported AEs were GI-related, occurring in 405/603 (67.2%) participants in the CagriSema 2.4 mg/2.4 mg group, 326/605 (53.9%) participants in the semaglutide 2.4 mg group, 60/152 (39.5%) participants in the cagrilintide 2.4 mg group, 329/594 (55.4%) participants in the CagriSema 1 mg/1 mg group, 288/608 (47.4%) participants in the semaglutide 1 mg group, and 42/149 (28.2%) participants in the placebo group. AEs leading to trial product discontinuation occurred in 51/603 (8.5%) participants in the CagriSema 2.4 mg/2.4 mg group, 40/605 (6.6%) participants in the semaglutide 2.4 mg group, 7/152 (4.6%) participants in the cagrilintide 2.4 mg group, 42/594 (7.1%) participants in the CagriSema 1 mg/1 mg group, 26/608 (4.3%) participants in the semaglutide 1 mg group, and 2/149 (1.3%) participants in the placebo group.2
In the REIMAGINE 3 trial, the most commonly reported AEs were GI-related, occurring in 51/90 (57%) participants in the CagriSema 2.4 mg/2.4 mg group, 42/93 (45%) participants in the CagriSema 1 mg/1 mg group, and 21/91 (23%) participants in the placebo group. AEs leading to trial product discontinuation occurred in 6/90 (7%) participants in the CagriSema 2.4 mg/2.4 mg group, 11/93 (12%) participants in the CagriSema 1 mg/1 mg group, and 1/91 (1%) in the placebo group.3
- Based on the efficacy estimand: estimated efficacy in an idealized scenario in which all patients stayed on treatment and without initiation of additional glucose-lowering medication.
** Based on the treatment regimen estimand: treatment effect regardless of whether patients stayed on treatment or took other glucose-lowering therapies.

Selskapet kjører en live webcast i natt (01:30) her:
https://edge.media-server.com/mmc/p/xxkg9u3t/
Her er slides:
Positivt! Får satse på at det forsetter
3 Likes
I webcall så sier nevner de også som grunn til høy discontinuation ikke nødvendigvis var pga bivirkninger, men at de ikke ville gå ned mer i vekt. De valgte å ikke eskalere dose som gjorde at de måtte avslutte trialen
1 Like
Nei, det er fordi at hvis de fikk bivirkninger som gjorde at de ikke klarte neste dose, så ble de tvunget til å droppe ut av studien. Ingen rom for å gå ned i dose eller skippe over 1/2 doser.
Reta sin fase2 studie hadde denne fleksibiliteten.
1 Like
Da har man 2 faktorer som har spilt inn på høy discontinuation, rart Martin Holst Lange kun nevnte det jeg skrev (mulig det blir for detalj fokus hvis han også skulle gått i det som nevnes i tweeten)
1 Like
Novo sin kommunikasjon er grusom, burde vært eksplisitt forklart i pressemeldingen. Investorer og markedet sammenligner Lilly og Novo sine studier med argusøyne, og når det er store variasjoner i designet, som påvirker resultatene i stor grad, så burde det fremkomme tydelig.
3 Likes
På den positive siden er det hyggelig å se Mike Doustdar presentere slides som dette;

Er litt av dette man har ønsket å se etter utskifte av tidligere ledelse/styre, selvom de forsatt har mye jobb igjen å gjøre. Fortsetter det slik så er det postivit
1 Like

Sier strekene at vi skal under 200 DKK?
Hips dont lie, hvis ikke 220 holder så kan det kapituleres skikkelig
2 Likes
Ships don’t lie either.
Hva om oljen og alt bare krakkelerer nå i sommer? Og tar med seg Novo og resten av markedet ned i dragsuget? Og så gjør Novo noen særdeles strategisk riktige kjøp nede i Hormuz-gropa? Da er det bare å rygge lastebilen inn. Ev. chartre en supertanker, selv til dagens rater.
1 Like
Nye CEO ser forretningsmuligheter utenfor kjernevirksomheten, Novo Tankers🚢
1 Like











