
Mr ULTIMO kjøper aksjer 
2 Likes
(Slettet)
LOL. Har ikke sett før nå at det er BU… BULLTIMO. Get it?
Hvem av dere er Ketil???
1 Like
(Slettet)
1 Like
Her var det virkelig mye “fundamentalt” stoff å lese.
Her er en tekstbasert versjon av spørsmålsrunden fra dagens webcast. Noe fagspråk har kanskje blitt skrevet ned feil så si gjerne ifra slik at jeg kan endre på det i etterkant. Jeg legger svarene skjult slik at ikke innlegget tar så stor plass. Hvis det er noe spesielt interessant kan dere sitere i et nytt innlegg og diskutere.
Ultimovacs Webcast Q&A - June 8, 2023
We can start with the following regarding the supportive analysis performed by the radiologist at the different sites, was the analysis performed in a blinded manner?
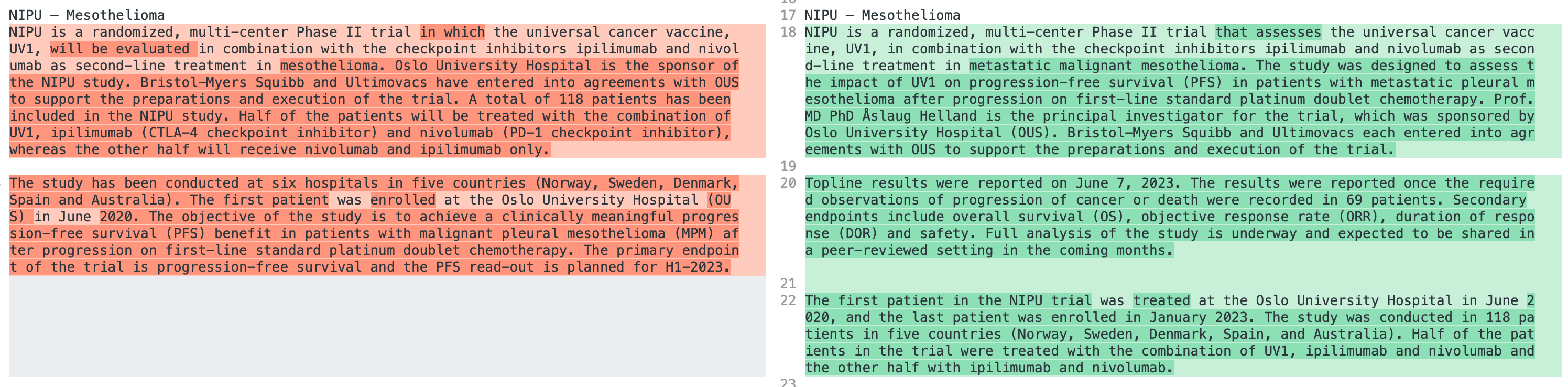
So this study is not a blinded study as such. So you can say that the central review will be a blinded review of the images. It’s a third party vendor that is looking at the pictures and assessing them. When it comes to local assessment of the pictures, there is no information as such going from the investigators to the radiologist at the different hospitals. But also there is a risk that there is information there that could give information so that they know what kind of treatment the patients received. So it’s a possibility for such information.
Remember that in this study, both arms, both the Ipinevo arm and the Uvon Ipinevo arm, are experimental treatment. Ipinevo is not approved as second line treatment for these patients. So it’s investigational for both arms. I also would like to repeat that this analysis, this local assessment of the pictures is a part of the primary endpoint. It’s a sensitivity analysis of the primary endpoint. And this is something that is predefined in the protocol.
Is it so that some studies use local assessment instead of central review to determine if the primary endpoints have been reached? If Ultimovacs had done that in the NIPU study, would the NIPU study then have met the primary endpoints?
Yes, this is always a difficult decision to take. So, as I just said, there is more confidence from the authorities in a central review. So that is something that is expected in a phase three. For example, if you want registration of the drug in this trial, it is also central review, as Mesotelioma is a hard to treat indication with few options for the patients. So it would be beneficial to have central review upon readout of positive results. On the other side, there is a lot of trials that use local assessment, not at least in phase two trials where you want to get information, as Carlos said, for further development in phase three. For both the central review and this sensitivity analysis. It’s the same statistics as we have disclosed earlier, with a hazard ratio zero six, one sided alpha, zero one, and a power of 80. And if the local assessment had been the primary endpoint in this study, the study would have been a positive trial So that’s correct.
Have you got the HR values? In case you have, why not let the market know the values?
It’s a very good question. And this was a dialogue with the investigative team. And basically the outcomes of that discussion was, as this team believes that they have very strong data to present a medical conference. Their preference was to disclose these HR values at that conference. What we can tell you. As we put in a press release and as Jens just mentioned, if the HR values in the local review would have been a very positive study with very strong statistics. Understand review, we didn’t meet the primary point, but as we mentioned, this is the preference of the lead investigator and they own the data. And of course, they want to make sure, because they believe that they have very strong data to get a very good presentation at a medical conference.
Despite not seeing a positive outcome in the primary endpoint of the trial, do you see a positive trend close to significance?
Again, we cannot comment on that because that will be good delays and that was the decision from the investigator to save those details to the conference. I just said basically, what was the results? If you look at the strength of the data, if you look from a central review or from a local review.
What was the cleaning time for the NIPU data?
Again, that’s a process that is not under our control. So that’s the investigative team that does that process and they have that information and it’s not important for us. How important for us is the data that we receive and that we will be receiving in full detail at the medical conference.
When do we estimate the detailed data will be presented at a medical conference?
The only thing that we can disclose, because again, this is the prerogative of the investigated team and Professor Åslaug Hellen, is that they are targeting a major medical conference and they will want to present again because they think that it’s a very strong date at a very good conference. So we will be able to inform you when they inform us which conference they receive. Acceptance to present.
If you state that overall survival is the gold standard for these types of trials, why did you choose PFS as a primary endpoint?
So at the time this study was discussed, back in 2019, it was very little information regarding the efficacy of CPIs in Mesotelema. So it’s important for us, for the investigators to understand as much as possible about the mode of action and also to have speed in the trial. You will reach, of course, PFS before you reach overall survival. So this was done to have a large or a lot of information on the patients within a relatively short time frame.
In this trial, as you know, the patients will be followed for three years for overall survival. So you will have the same overall survival information in this trial as if the endpoint was overall survival. And since this is not a registration study, we have not now had the opportunity to have a readout of clinical data unless we had to wait a bit longer for the overall survival to mature as we are doing now after the readout of the PFS.
Then I will ask two questions that are closely related. Given how the study was powered, do you think that a statistically significant PFS improvement in the treatment group was likely? And the second question, considering how the study was powered, could you discuss potential differences between statistically significant and clinically relevant PFS differences?
Yes. So in this area, in the Mesoteliome area with CPI, there is no, at the point where this study was discussed, there were no randomized data that we could use to really understand how the CPIs are behaving within this cancer indication. We had, after a while, information from first line data. So what you do, so you go to the clinic and ask the investigators, discuss what is seen as a relevant clinical efficacy from a new drug, and then you need to work your way backwards into the phase two trial. So a hazard ratio of 0.6 is something that is considered by the investigators and also accepted by the authorities when they approved the study to be a relevant level of the hazard ratio.
As you know, in phase two, the other statistics is not that tough as it will be in a phase three trial. So one sided alpha of 0.1 and Pover of 80 is quite common in these trials. Based on a positive readout of such trials, either with the PFS here as a primary endpoint or even the gold standard endpoint overall survival, this will be something that will give us confidence to move on in the Mesotelioma trial.
How likely is it that patients will go on to try different treatments after progression? Assuming that some will, how do you view the overall robustness in the overall survival data going forward?
Well, so, just to remind, in this indication, there has been first line treatment with the chemotherapy only until quite recently. And over the last few years we have seen the entrance of CPIs with the Epinevo, as you know, in first line treatment and also over the last year where they combine CPIs with the chemotherapy. So for first line treatment, there is established standard of care in the second line of this cancer form. There is no obvious standard of care in the market. So most likely patients receive palliative chemotherapy for several rounds, one, two, three rounds after progression, after first line treatment. So there will be patients that receive of course, new treatment after progression.
In this study, we expect this to be distributed equally to both arms, so this will not impact how we evaluate the overall survival data. This is of course something that happened in all trials and just as a reminder, this will be even more drugs if this was an earlier phase trial. In the end, I just want to say that you need to do overall survival to get the registration for the drug. So it is understood and expected that patients will have been exposed to also other drugs after a trial is finished.
While you are not sharing any numbers, can you say anything about how large the difference between the two radiological assessments was?
I think I answered the first part of that earlier on. I think we had a similar question. And regarding the difference to what I can say again, or as much as I can say the rest is for the details when the investigators so decide is that, and we already have several times if the study would have been measured in the primary endpoint under local review would have been a very positive trial with highly significant statistical differences. But Anderson’s review, we didn’t meet a primary endpoint. So it’s as much as I can say I can understand the curiosity, but that more details will have to be dependent when the lead investigator will decide to share that information. And again, as I said, their goal is to be presenting the strong data at a medical conference.
Are you going to ask for a new independent central review?
Well, no. What you do here so remember that what you are trying to do here is to really help patients with a very severe form of cancer and you try to do that as objectively as possible. The central review is something that is predefined how it should be conducted and you follow a lot of rules within the resist system to get the answers true. This is an independent review of the slides. So in that word it also lies that this is the view of that third party vendor. It’s also here conducted a local assessment of the images, which is different from the central review. And of course, in the light of giving as best diagnosis as possible to the patients moving forward, the group will assess and try to understand where the differences is so that this can be discussed and developed further in the future. So no new independent review, but there will be attempts to understand the differences in the review of the slides.
And just to give another comment here, and the comment from the investigators is that they understand this difference. But for them, the important and for the authority is going to be what is going to be the final number or the more information on overall survival, because reviews are a little bit subjective depending on the radiologist, but overall survival is very clear. And really that’s the part where they say so far is a very positive trend. And for them, that information overall survival, as Ian’s mentioned several times overrides the PFS from the perspective of deciding the next step in the development of UV One and the indication.
Have you received any feedback from the checkpoint inhibitor sponsor BMS about this top line data?
BMS was with us when the investigating team shared the data. We were of course present and BMS was also participating. So the data was shared with both companies and of course we are talking about that, this was shared yesterday. So I’m sure BMS will do their internal review and process. I can just say the comment was that this is not unexpected. They have a lot of information and as they said, also from their experience, PFS is probably not the best endpoint, but besides that, it’s for them and they will do the internal review, but they have the same level of data that we have.
Is the shown efficacy signal enough to initiate a phase three trial in this indication? And also another related question, will you pursue a phase three trial in Mesothelioma?
The data’s confidence, the investigative team is very supportive using the data to proceed. Of course, as a company we are positive about this data, but we believe of course that it makes absolute sense because to wait for the presentation of the full set of data at a medical conference, because that’s the data we will have to bring to the authorities to discuss the next steps in the development. But for the time being, let me just say that there’s no reason not to think that pursuing Mesothelioma is part of our objectives.
What was the separate predefined local assessment target compared with target for primary endpoint met?
I’m not sure if I completely get the question, but I guess it’s around the statistics. The statistics as mentioned earlier in this trial was a hazard ratio, six one sided alpha of 0.1 and a power of 80. And this statistics goes for both the primary endpoint and an analysis around that endpoint. So for the local assessment it was the same statistics as for the primary endpoint. I think maybe just to clarify, because we get a lot of these different questions, as Jens mentioned, the statistics plan is the same. The images, the radiographic images are the same.
The only difference is that where are the radiologists that assess those images?
They are in a CRO as a center review or they are the specialists and experts in the hospitals that participate in the study. That’s the only difference.
Was the central radiology review done at the end of the study or was it done in parallel with the local review?
So for central reviews of the images is taken at the different hospitals of course and then they are sent off to the third party vendor, they have their internal set up how to review the images to get good quality on the results. This is an ongoing process throughout the study and it’s also a process where the CRO in collaboration with the study ensure that they receive all the pictures taken from the patient so they can have the full story about images from each patient. But this is an ongoing evaluation of images.
Health Talk is basically stating that Hasser ratio is one for the NIPU trial when saying experimental arm did not survive any longer than control arm. Is this correct?
Jans can comment, but I don’t know if Talk if first it makes that conclusion and how can they make that conclusion? Because as a ratio doesn’t measure PFS, doesn’t measure survival so I don’t think if that even the question is correct or the text. So again, acid ratio measures progression free survival the time that it takes for patients to progress or die overall survival is a totally different endpoint and assesses at regular points in times how many patients are alive in the different items. So the other ratio doesn’t apply in this case as primary endpoint to overall survival.
But Jens, I don’t know if you want to no to just reemphasize what you said now. So the statistics in this trial is for PFS and that is the primary endpoint after 69 endpoints. We have now had a readout of that with a different analysis, a central one and a local one with different results. We do not have the numbers. Further, all patients in this trial will be followed over the next years for overall survival for the overall survival data to mature and that is what we are waiting for in this trial. Last yesterday we were informed that as of now there is a positive trend in overall survival. The data need to mature to get a more statistic information on the difference between the two groups of patients. So in reality it’s the opposite. So regarding overall survival, the information we have is that there is quite an important positive trend in favor of the UV one arm versus the control arm for overall survival.
Do you have any information on potential subgroup stratifications for instance PDL one status as no, we do not have that information. It will be disclosed at the presentation at a conference in the future. Okay, so one question can we expect the same kind of bad result with initiation?
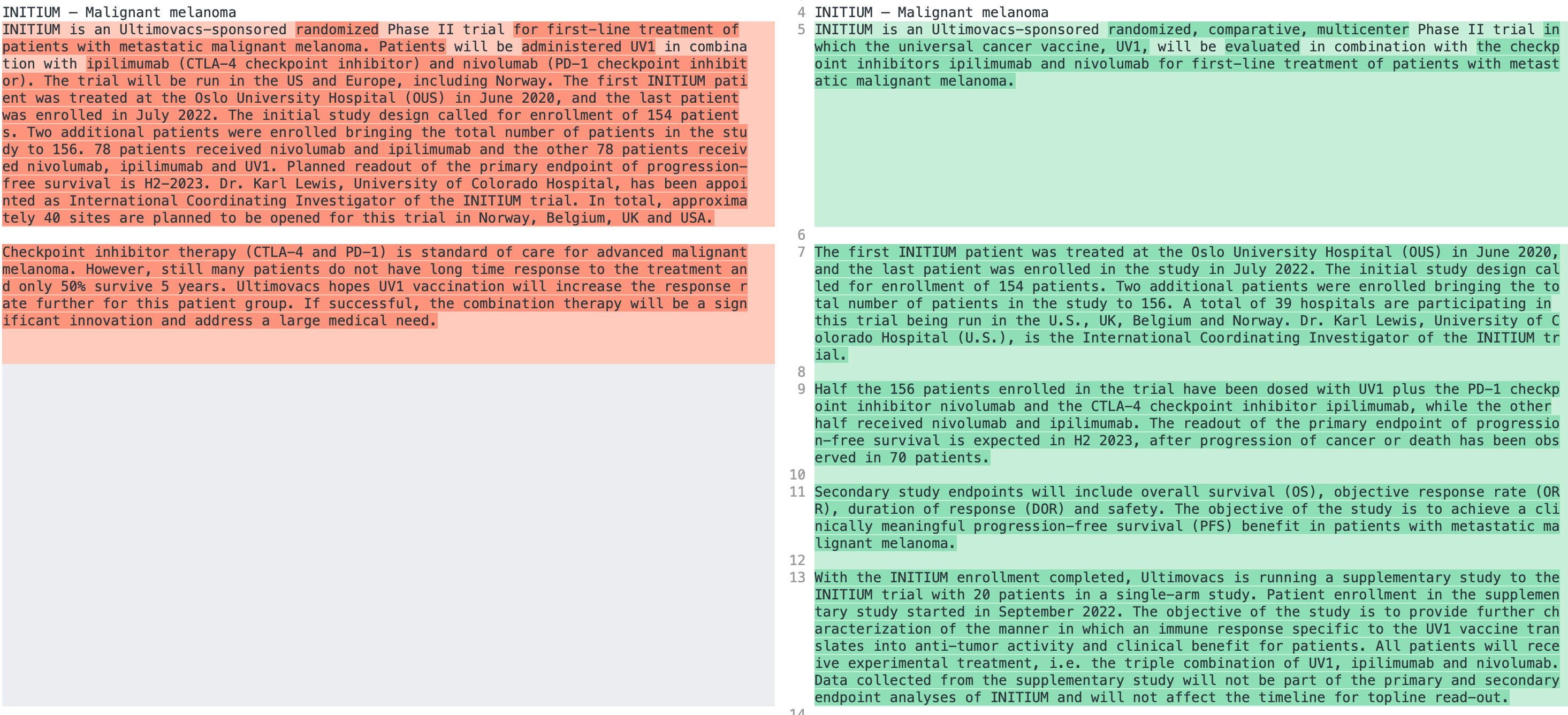
First, a couple of comments. Again, we don’t consider this a bad result, we consider this and that the study didn’t meet the primary endpoint from a statistical perspective as previously defined. We believe that we have good data shared with us by the investigators that are supportive and initium. As in melanoma is a totally different type of tumor, totally different biology, where clearly the checkpoint inhibitors have a totally different level of efficacy. That is very well defined in mesothelioma. This was the first study that we did where we had information in mesothelioma and again in probably the most challenging group, that is the second line mesothelioma. In melanoma we have very supportive information from the phase one, we know that in initium treatment is having an impact by delaying the progression or death in these patients.
So first, we don’t consider this a bad result and second, there’s no way of moving these results again to an issue. As a matter of fact, we think that the data that we were exposed to support and lead us to be more optimistic in terms the impact of UV One in these other indications and particularly the next one that we’ll expect, that is melanoma. Just to add a comment here, if you view the history of clinical trials in Ultimovacs. So we have conducted several phase one trials earlier and based on those results from those trials and information in the market at different time points, we selected as a company Malignant Melanoma as our sponsored indication.
So our lead indication here is Malignant Melanoma. Over the last years we have presented Ultimovacs in different conferences and in different ways to different environments and we are very happy that we have received a lot of interest for the vaccine over the last years. So, in total, as you know, we are participating in four investigator initiated trials when we develop UV One, and I think this is important. We are, of course, developing UV One and hope that this will be of importance to patients. Right now, in the development of cancer vaccines, nobody has the full insight in how a vaccine work in connection with checkpoint inhibitors. As you can see from the different trials we are part of or sponsoring of, there is very different biology in different cancers.
For the mesotelioma and the head and neck cancer, there is a low expectancy from the CPIs when it comes to efficacy. For patients on the other side, in nonsmall cell lung cancer and malignant melanoma, it’s expected to have a huge impact to give CPI to patients. To really understand how a vaccine works, when you combine that to the checkpoint inhibitors, we need to be in different biologies. So for us this is very important information to see how. The vaccine behave in different biologists, difficult to treat patients like the mesotelioma and hedonic and also how it works and what it possibly can add to already quite good results with CPI, for example, in melanoma and nonsmall cell lung cancer. So I think it’s important to reflect also on this. It’s important for the development of the field and how the vaccine works to be brave enough to participate in different indications, which might not be obvious, a home run in all indications, but it will contribute a lot to the scientific community and hopefully for the patients in the end.
We have a question that is related to what you shared now. So I will ask that and you can consider if there is something you would like to add on top of what you just said. Given that you say you will develop a universal vaccine, will you now put the ambition of a universal vaccine on hold?
This is an interesting question in a way. So when we are saying that an antelomerase vaccine is a universal vaccine, you can view that from different angles. So one angle is that is this an antigen that is relevant for different indications for patients with different forms of cancer? And to that we can answer yes. If the immune system get interested in telomerase as a target, this is a relevant target in 80% to 90% of all cancer indications. When it comes to stage these days, there’s a lot of discussions around earlier stage of treatment versus later stage of treatment. The telomerase expression as such is something that starts, it starts to express telomerase early on in the cancer development and it’s present throughout the course of the cancer. So you will see expression of telomerase from early stages to late stages, both in the primary tumor and in the metastases. Another way to look at the universality of this vaccine is to look at who can get this vaccine. So in the telomerase peptides, there is several different epitopes that can be recognized by different HLA classes around the world. We have looked into this and we believe that this has a global coverage. We do not do any HLA screening of patients prior to inclusion in studies and expect a good immune response in different territories.
Just a reminder, in our earlier trials we had an immune response between 80 and 90% in the different phase one trials. So when it comes to the clinical universality, that is a different question. So imagine that the vaccine, the mode of action of the vaccine is that it add effect on checkpoint inhibitors, right? So for example, in melanoma you expect response rate in patients around 50%. So 50% of the patients will, when they receive checkpoint inhibitors, they will have effect. And what is that effect? The effect is that the CPIs is opening the tumors and the draining lymph nodes so that the preexisting immune system can kill the cancer cells. If the checkpoints were effective for more than 50% of patients in melanoma, it is likely that also the immune system could have an effect on those patients. So, putting this into context, it’s actually two different mode of actions here. One is the vaccine mode of action. We are injecting the vaccine, we are generating T cells that are designed to kill off the tumor cells in the end. But these T cells need to have access to the tumor. So therefore you combine with checkpoint inhibitors so that the T cells can enter the tumor and the draining lymph nodes. This is one part that could be discussed when it comes to universality, but the universality also lays on the checkpoint inhibitors. So we do hope that in the future there will be a development of even new checkpoint inhibitors that open the tumor for the immune system in even more patients.
And as we have stated over the last years, we see the CPIs as our collaborators. We want to combine with different CPIs that show this effect that the tumor is opened for the immune system. Another mode of action, just very short at the end here, is that there’s something that we call the cold tumors and that could be different things. But if you define that as a tumor that does not respond to the CPIs, this is also an interesting area for us to understand. If a vaccine, for example, the UV One vaccine, can change the microenvironment in these tumors, so that also these patients have efficacy from the checkpoint inhibitors. As you might remember from the 103 trial, we have just presented data on that one we saw in the overall group and in the group that were PDL One negative, the same results. We acknowledge that that was only 30 patients, but that is kind of information that is important for us moving forward. In the Mesotelioma trial, which is the trial we discussed today, there is a very small group of patients that respond to CPI, meaning that there is a small group of patients where the immune system get access to the tumor and have clinical efficacy.
For most patients within mesothelioma receiving epinebo, they will progress immediately because the Ipineibo have no effect on those patients. What we try to understand in this study is also if the vaccine on top of Ipinebo can move, the patients from being responsible, don’t respond to the CPIs to be responders when you add the vaccine on top. So it was a long answer to that question, but this information is the reason why we are in the different indications. So we want to explore the mode of action in different biologies. As I stated earlier, I also want to take the opportunity to clarify some misunderstanding, because the question makes the assumption that we consider mesothelioma as a failed indication that we miss an indication that is far from being true. The fact that again, let’s remind us is a phase two study PFS is just the primary endpoint and it’s not the full information of the study. As I mentioned, based on the information that we have and that of course we will have full detail later on, there’s no reason not to think that Mesothelioma is a valid indication to further develop using UV One, but of course, most naturally in first line. So I want to clarify that from our perspective, the fact that we didn’t emit the primary endpoint persons review doesn’t mean that this is a failed study. On the contrary, we think that the data is quite supportive for Mesothelema patients and also for giving us additional information for the rest of the program.
Could the commented data from the Keynote 483 study which MST released in March, does this result have any impact on the further studies with UV One in Mesothelioma?
Well, so as I said earlier, over the last few years now this field or patients with Mesothelioma that earlier were treated with only chemotherapy, now have access to CPIs. First with the Pineva trial and different companies now develop the CPI in connection with the chemotherapy. We have seen some of these results now recently, and it seems like the Epinebo combination and the CPI chemotherapy options have roughly the same overall survival in these patients. There are still some results to wait for in this field and how it will end up. What will be the standard care is as of now, not completely understood, but one thing that is certain is that in this field, moving on, there will be CPI for patients, meaning that the immune system will be involved in treatment of these patients. Also in this field, even if it’s very early, there’s also discussions how to move the treatment earlier. So there is also a lot of initiatives where they test the CPIs in the Adjuvant or Neoadjuvent setting the most. So CPIs will be around. What the standard care will be in the near future is still to be decided, but it’s obvious that they have moved away from only chemotherapy for these patients in the society. And of course this expands the potential for UV One to have more combinations. So, as Ian mentioned, the more the CPIs are used, the more we see opportunities to use UV One in combination with CPIs.
Only a tiny minority in the market has acknowledged that the threshold for reaching the primary endpoint in NEPU was a hazard ratio of zero point 73. Would it not be relevant to state this number in the press release?
So the statistics in this trial, and I’m not a statistician, just to be precise on that. So, as I have mentioned earlier, the theoretical statistics, the background for these studies is this alpha 0.1 power 80 and has a ratio of six. When you then start a study and then look at the results afterwards. If you are below 76 in these trials, you will have a positive study, meaning a p value below zero, one sided alpha. So I do think that we have mentioned this in some earlier presentations, but yes, this is something that we will bring on further in presentations.
At which medical conference is the principal investigator aiming to present this data on?
We are not at liberty to disclose that. That is really a decision and responsibility from the lead investigator. When Professor Åslaug Hellen wants to disclose that, she will do it, but the only thing we can tell is that they really target a major medical conference.
The interpretation of primary endpoint met at the local hospitals is that point of view shared by all hospitals taking part in the study. So what happens with the local assessment?
So in the local assessment, the images taken at the hospitals are reviewed by the local radiologist at these different specialist centers and they are informing on their results in the database. When all information is in the database from all images, this information will be used by the statistician in the study to calculate the different information needed and the primary endpoint. So there is no discussion or review across the different hospitals to understand if they have the same view on the pictures. So this is a result where the different hospitals contribute with the data and afterwards that data is calculated and endpoint presented as we have done.
Commenting on the statement that this does not need to be the end of UV one in this indication, what can we expect in terms of time before decisions on the way forward will be taken? And we also have another question that we can add. It may have been answered, but at what time can we expect to have this more mature data presented?
Well, I think we already addressed that. Basically, investigators, again, as I said, they believe that they have very strong data, they want to present it at a medical major conference. So I’m sure they don’t want to spend too long on that. What I can say is that although we are positive in pursuing the indication, of course we need to wait for that data. So a decision and a plan to move forward is going to be dependent on us having access to all that data to share with the authorities and discuss the next phase of development. So one way is linked, one decision is linked to the other. But again, their plan is to present as soon as possible at major medical conference.
As 69 patients have had progression, what would be a good result for this population in terms of progression per arm? And specifically, would 30 30 progressions versus 39 be seen as a good result?
Well, we have discussed this also earlier. So just a few words on the statistics in these trials, both in the NIPU trial and in the initial trial. So what is done here? So you use historical data. It was not that much historical data in the mesotelioma space in second line when we started this trial. But you use historical data to try to get the gris. How many patients is needed in the study and based on what you, the investigators or us in the initial trial decide as a relevant hazard ratio target, the number of patients is calculated, then you need to decide how certain you will be about the result. If you have tough values, you need more patients. In a phase two, the statistics we have is a common statistics in tribes. And then you start a trial with the two different arms, and you wait for those endpoints to occur. In this trial, 69 endpoints. And it’s the area between the curve, the I axis and the x axis versus the other curve, I axis and the x axis. That is, in a way, defining the hazard ratio in the study. So two things are important there because I have seen a lot of discussion around how many patients do you need in the different arms. There are one more thing that is important and that is the time to progression. The time to progression will impact on the area under the curve. So it’s both the number of patients in each arm but also how long it took for a patient to progress. So in extreme circumstances, there don’t need to be too many patients difference between the two arms if they progress at very different time points.
One question I would like to comment on myself as CFO. It reads the stock price is down over 30%. Do you think this is an overreaction?
As a general comment, we never will make comments about the share price or Ultimovacs, so we don’t have any comment on that.
The next question, there are two different questions on the same topic. Have you reached 70 end points in initiation by now or is it waiting? And another one, can you inform about the number of events by now in the initial study as informed?
We will keep all the market updated regarding initium at different point in time. And so we are not going to disclose at this time any information about that. We maintain the previous information that we expect the top line results for the initium study to come in the second half of 2023. And if at any point in time we believe that there is enough information to change that guidance, then we will inform the market accordingly.
Is it possible to explain more about why these NIPU results are also positive instead of focusing on the differences between local and central review?
So the most important endpoint for these patients is of course survival, that you treat the patients so that they survive for a longer time and that is the most important thing and that is the ambition in all cancer development to keep the patients alive. So PFS in this study is surrogate endpoint that is there to if you see an association between improved PFS and overall survival, will inform on overall survival for doctors and in future clinical studies. So the PFS is an important endpoint, the overall survival is even more important. And what we see in this study is that there is a trend, a positive trend in this study for overall survival in the arm with patients that receive UVone, eplibumab and Iblimab. As you recall, the last patients were included in the study just months ago in January, was the last patient enrolled. So this data need to mature somewhat longer to get a good understanding of this trend. This is something that we see as positive, that this is stated to us from the investigators that they see this positive trend and we are encouraged to follow over the next time to see how this develop. Also for the PFS, the primary endpoint was negative, the local assessment was positive. That is a pity and it is of course somewhat harming the development in the short run, but we believe that in the long run, when this data mature, we can take a good decision and to move further on into phase three and development. In this indication, we would have needed overall survival also. In that circumstance, we would never start a phase three trial based on PFS data only. So in a way we have got more information on the overall survival. We know that there is a trend now. We didn’t know that a few days back. Yes, it’s a pity that the primary was negative, but in the long run it’s the overall survival that we need to have there to make a decision for the further development. And we are at the moment positive about the information we have received.
45 Likes
Jeg tviler på at Helland hadde vært med på formuleringen om at de fikk “endpoint met” i sin analyse av resultatene uten at hun er helt sikker på dette. Har sjekket ReasearchGate, og hun er referert 9000+ ganger og en h-indeks på 50 (nobelprisvinnere ligger typisk rundt 30), så fallhøyden er stor ved å uttale noe som er faglig feil.
Basert på det har jeg antatt at de fikk noe som er ekvivalent med 39 events. Med 8 ukers QC blir det:

41 Likes

Redeye ute med sine kommentarer
Konklusjon:
After much discussion above, we leave our estimates largely unchanged, pending more quantitative NIPU data. We estimate investigators to present more granular survival data at a medical congress in late 2023e-2024e. Still, we delay a potential market approval for a UV1 and CPI combination therapy in mesothelioma from 2027e to 2028e in our model, considering a likely longer time from phase II top-line data to starting a potential phase III trial. Further, we trim our estimated likelihood of approval for UV1 in mesothelioma from c20% to c18%, reflecting slightly higher uncertainty in this indication. Lastly, we update our future capital raise assumptions.
Reflecting these estimate changes, we lower our base case from NOK129 to NOK127. Further, we decrease our valuation range from NOK43-213 to NOK36-210.
Interessant lesning.Som en liten teaser:
"Independent, blinded review represents the gold standard for clinical trials, and regulators usually require this setup for phase III trials. We believe that the local, unblinded investigator reviews, at least somewhat biased, should be taken with a tablespoon of salt. "
6 Likes
I tilfelle denne ikke er nevnt tidligere og andre også har lyst til å lese seg litt opp på hvor vanlig det er å se diskrepans mellom local lab og sentral lab mtp CT bilder.
For mesoteliom vil jeg gjette at det er endel vanskeigere
6 Likes
Akkurat dette poenget har druknet litt i bølgene - men det beskriver nok situasjonen i et nøtteskall:
Når primærendepunktet ikke ble offisielt nådd OG det oppstod faglig uenighet om det er riktig vurdert SÅ har Helland og teamet vurdert det slik at DE vil ha full regi på hvordan denne uenigheten best presenteres sett fra deres side slik at fagmiljøet som de tilhører (de bryr seg ikke om markedet) ser verden best mulig fra deres side.
Det er for meg lett å forstå hennes standpunkt her - dele så lite som mulig i en markedsbasert/selskapsdrevet presentasjon som Helland ikke ville hatt full kontroll over - fordi hun da ville risikert at kruttet hun sitter på likevel druknet i markedsstøyen, samtidig som hun ville mistet cred og kanskje mulighet til å legge frem caset slik hun ser det på neste store forskerkonferanse på høsten.
Svaret får vi på høsten - da ser det for meg ut som det kommer en kraftig rematch der hun vil hardt argumentere for sin resultatforståelse av PFS - og hvis OS i mellomtiden også har gått i hennes favør - så kan det komme en kraftig reprising da. Litt avhengig av hvordan dette filtreres ut i mediene også. For akkurat nå er det nederlagsoverskriftene som sitter igjen, ihvertfall for de fleste som ikke er dypt inne i caset.
Men det er jo derfor selskapet hele tiden har vist til - på inn og utpust - at dette var en forskerdrevet studie som de ikke hadde kontroll over - ikke fordi det er ment defensivt og kanskje var feil indikasjon å kjøre frem først sett i ettertid, men fordi de vil ha frem slik CEO til slutt sa rett ut i sitatet over på Q&A - uenigheten er sterk og nå sikter de mot «a very good presentation at a medical conference» (les: Helland har gått i flint og skal sette skapet på plass selv, alle andre selskapshensyn, inkludert kursutviklingen i mellomtiden er underordnet).
Maybe.
Så er spørsmålet bare om vi kan få live streamet den presentasjonen. Det hadde vært gøy.
28 Likes
Vi har fått bekreftet av IR at ledelsen i Ultimovacs og representanter fra BMS fikk se topplinjedata.
Vi vet videre at:
- Studileder mener at primærendepunkt på PFS ble oppnådd. Hun er tilsynelatende sikker i sin sak fordi uenigheten tillates skrevet eksplisitt i meldingen og det er bedt om embargo for å få maksimal impact på kommende konferane (ESMO til høsten)
- Studieleder forteller at de observerer en forbedring i OS i UV1-armen vs. kontroll (men at disse dataene nødvendigvis må modnes noe mer)
La oss så anta følgende gitt det ovenstående:
- HR-verdien var (svært) nærme hverandre i vurderingene til henholdsvis Independendent Review Board (IRB) og studieleder
Det er vanskelig å anta annet enn at man nå har en situasjon der UV1 gir en HR-verdi som er nærme 0,73. Om du spør studieleder som har en av de høyeste stjernene i det kliniske miljøet, så er HR-verdien lavere enn 0,73.
Mitt spørsmål er da, etter å ha topplinjedata, hva gjør BMS ? De kjenner Ultimovacs og Helland godt. De ville sågar i utgangspunktet at NIPU skulle ha høyere power og rekruttere flere pasienter. Noe som fort kunne gitt et annet, omforent positivt utfall i denne studien.
Før vi fikk resultatene var de fleste enige om at en HR på ~0.8 eller bedre er godt nok for å utløse ønske om fase-3 og/eller andre initiativ fra pharma (her: BMS). Denne situasjonen har vi nå fått. Gitt at denne antakelsen stemmer, hvor raskt kan BMS finne på å bevege seg? Ønsker de å vente på ESMO og mer data fra Helland?
10 Likes
Det du skriver her er at Radforsk med styreleder Einarsson og en annen innsider i går handlet aksjer på med tilgang på informasjon som resten av markedet ikke har.
Er du virkelig sikker på at det er slik?
Dette høres ikke ut som måten det bør gjøres på, da er det mange aktører der ute som begynner å bli vel tvilsomme i sin atferd. Men det er absolutt et godt signal, men ryddig er det ikke.
1 Like
Styreleder har ikke sett data. Ledelsen (CEO og CMO) har sett data, dette er bekreftet av IR i dag.
5 Likes
Hvordan leser du dette ut av meldingen? Helland refereres da med sitat i meldingen på at primærendepunkt på pfs IKKE ble nådd, men at studien likevel viste statistisk signifikant effekt. mener du de to tingene er det samme?
1 Like
De to tingene er det samme. Det ble bekreftet i callen (sjekk ut Q&A) ovenfor. Et “positivt resultat” i dette henseendet betyr oppnådd endepunkt.
Is it so that some studies use local assessment instead of central review to determine if the primary endpoints have been reached? If Ultimovacs had done that in the NIPU study, would the NIPU study then have met the primary endpoints?
For both the central review and this sensitivity analysis. It’s the same statistics as we have disclosed earlier, with a hazard ratio zero six, one sided alpha, zero one, and a power of 80. And if the local assessment had been the primary endpoint in this study, the study would have been a positive trial. So yes, that’s correct.
As we put in a press release and as Jens just mentioned, the HR values in the local review would have been a very positive study with very strong statistics.
3 Likes

IRB kan like gjerne gjøre klar papirer for å melde oppbud når Åslaug går på scenen på ESMO og banker sine PFS + OS i bordet. Håper for pasienter og vår del at det virkelig er signifikante data som hun selv sier.
Neida, de får vel leve litt til 
3 Likes
Hvor kan man se bekreftelsen fra IR at CEO og CMO fikk se topline data?
1 Like